Biomechanical Reconstruction of the Medial Longitudinal Arch
An active, foot-core paradigm for the rehabilitation of adult functional pes planus — replacing passive orthotic bracing with neuromuscular re-education, intrinsic muscle hypertrophy, and closed-chain kinetic integration.
Foot Core SystemActive SubsystemFunctional Pes Planus12-Week Protocol
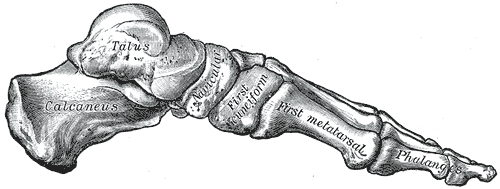
Skeleton of the right foot, medial aspect. The medial longitudinal arch is the curve formed by the calcaneus, talus, navicular, three cuneiforms and the first three metatarsals -- visible here in its unloaded anatomical state.
Source: Gray's Anatomy (1918), plate 290 -- public domain.
01 — Paradigm
The Science of Adult Foot Plasticity & Mechanobiology
The clinical assumption that the adult foot cannot undergo active structural modification is a pervasive myth unsupported by contemporary mechanobiology and neuromuscular physiology.
The clinical management of adult pes planus has historically been dominated by passive interventions — rigid orthotic insoles designed to mechanically brace a collapsed arch. Contemporary clinical biomechanics and physical therapy research has shifted toward an active paradigm: the Foot Core System. This paradigm asserts that the human foot is not a static, immutable structure once skeletal maturity is reached, but rather a dynamic, highly adaptable biomechanical organ capable of functional and structural remodeling.
Through targeted neuromuscular re-education, intrinsic foot muscle hypertrophy, and closed-chain kinetic integration, adults presenting with functional (flexible) pes planus can systematically reconstruct their arch, alter static postural alignment, and restore efficient gait mechanics.
While skeletal maturation is complete by the end of the second decade, the muscular and tendinous components of the foot retain a high degree of neuroplasticity and morphological adaptability throughout adulthood. The medial longitudinal arch (MLA) is dynamically supported by the active subsystem of the foot core — four layers of plantar intrinsic foot muscles (IFMs). When targeted with progressive mechanical overload, these muscles undergo:
Increases in cross-sectional area (CSA) and muscle thickness
Enhanced motor unit recruitment and firing frequency
Improved baseline resting tone and active tension-generating capacity
Elevated passive stiffness of the plantar fascia through the windlass mechanism
Reduced excessive navicular drop and corrected rearfoot valgus alignment
10.6%
Median increase in abductor hallucis CSA after 10 weeks of minimalist shoe walking — matching clinic-based strengthening outcomes.
0.26 cm²
Median CSA gain in AbdH after only 4 weeks of Short Foot Exercise, directly correlated with Navicular Drop Test improvement.
4–8 wks
Time-to-significant-hypertrophy in AbdH, FDB, and FHB under consistent isolated IFM training.
9% ↑
Increase in activation of the Flexor Hallucis Brevis during SFE; significant muscle thickness gain over 6 weeks.
Translational takeaway: The data does not support the long-standing belief that adult arch structure is fixed. When properly loaded, intrinsic foot muscle morphology responds on the same timescale as larger postural muscles — and integrates into real-world gait via minimalist footwear exposure.
02 — Anatomy
The Foot Core — Four Layers of Intrinsic Foot Muscles
The active subsystem is organised in four anatomical layers. Local stabilisers of the medial longitudinal arch sit in the superficial layers; deeper layers control fine MTP kinematics and modulate the pull of the long extrinsic tendons.
Layer 1 · Superficial
Abductor Hallucis · Flexor Digitorum Brevis · Abductor Digiti Minimi
Direct medial arch support, plantar pressure distribution, hindfoot pronation control.
Layer 2 · Intermediate
Quadratus Plantae · Lumbricals
Standardises FDL tendon pull; prevents calcaneal eversion and arch collapse; fine toe control.
Layer 3 · Deep Flexor Hallucis Brevis · Adductor Hallucis · FDMB — MTP flexion of the hallux; first-ray stabilisation during propulsion.
Layer 4 · Deepest Plantar & Dorsal Interossei — MTP stabilisation and transverse arch contribution during toe-off.
03 — Evidence
Hypertrophy & Adaptation Metrics
High-resolution musculoskeletal ultrasound and MRI studies have quantified the morphological adaptations of each intrinsic foot muscle to targeted training stimuli.
Intrinsic Muscle
Plantar Layer
Primary Biomechanical Role
Hypertrophy & Adaptation Metrics
Abductor Hallucis (AbdH)
1st (Superficial)
Abducts & flexes the hallux; directly supports the MLA; controls rearfoot pronation.
10.6% CSA hypertrophy in 10 weeks of minimalist walking; significant increase in active motor unit recruitment (EMG).
Measurable increase in EMG amplitude and CSA with minimalist shoe walking protocols; lateral column stiffness improvements on toe-off.
Adductor Hallucis (AdH)
3rd (Deep)
Adducts hallux; stabilises transverse arch; counterbalances AbdH during propulsion.
Increased contractile shear modulus on elastography following intrinsic training; key to transverse arch integrity during single-leg stance.
Lumbricals
2nd (Intermediate)
Flex MTP joints while extending PIP/DIP; prevent claw-toe deformity; fine-tune arch dome tension.
Reduced clawing and improved toe dissociation within 2–4 weeks of toe-yoga drills; motor control gains precede measurable hypertrophy.
04 — Diagnosis
Clinical Differentiation: Flexible vs Rigid Pes Planus
Prior to initiating any arch-rehabilitation protocol, it is clinically mandatory to differentiate between functional (flexible) and structural (rigid) pes planus.
Flexible pes planus is characterised by a structural collapse of the MLA that occurs exclusively under weight-bearing conditions, whereas a rigid flatfoot displays a flattened or absent arch in both weight-bearing and non-weight-bearing states.
Rigid flatfoot often stems from congenital anomalies, bony coalitions (talocalcaneal or calcaneonavicular bridges), or advanced osseous degeneration, making it largely unresponsive to neuromuscular training and requiring surgical or orthotic management. Conversely, flexible pes planus represents a functional deficit in the active and passive subsystems — rendering it highly treatable through corrective exercise.
Mandatory screening step: The three assessment tools below — Navicular Drop Test, Jack's Test, Feiss Line Test, and Tip-Toe Standing — together distinguish a trainable flexible flatfoot from a structurally rigid one. Skip this step and you risk loading a coalition or degenerative joint.
05 — Assessment Battery
Clinical Assessment Procedures
Four validated clinical tests — used in combination — reliably distinguish flexible from rigid pes planus and quantify functional arch deficit.
The Navicular Drop Test (NDT)
A highly reliable clinical assessment tool used to quantify the degree of functional foot pronation. Direct vertical measurement of the navicular tuberosity from subtalar neutral to fully relaxed weight-bearing.
Jack's Test (Hubscher Manoeuvre)
A static, weight-bearing test designed to evaluate the integrity of the passive windlass mechanism and assess the flexibility of a flattened arch. Passive weight-bearing dorsiflexion of the hallux at the 1st MTP joint while observing the MLA and calcaneus.
Feiss Line Test
A line is drawn from the apex of the medial malleolus to the center of the first MTP joint. The position of the navicular tuberosity is then assessed relative to this reference line under full weight-bearing. In a normal arch the tuberosity lies on or near the line; its descent is graded from Grade 1 (one-third distance to floor) to Grade 3 (touching the floor).
Tip-Toe Standing Test
Evaluates arch reconstitution under active loading. When the patient stands on their tiptoes, a functional flatfoot will demonstrate immediate arch elevation and calcaneal inversion; a rigid flatfoot will remain locked in eversion.
Arch collapses under load, then reconstitutes visibly during hallux extension.
Arch remains collapsed; hallux extension fails to lift the arch.
Feiss Line
Navicular position vs. MM–MTP reference line.
Tuberosity on or slightly above the line.
Tuberosity below the line — Grade 1, 2, or 3.
Tuberosity resting on the floor (Grade 3) regardless of weight distribution.
Tip-Toe Standing
Active unilateral heel raise.
Symmetrical arch rise; heel shifts from eversion to inversion.
Flat arch reconstructs into a visible symmetrical dome on heel-lift.
Arch remains flat; calcaneus fails to invert — often exhibits compensatory eversion.
06 — Gait
Normal Gait Biomechanics & the Windlass Mechanism
An active, functional foot core operates as a dynamic transformer during the walking gait cycle — transitioning from a compliant shock-absorber to a rigid propulsive lever. This tri-planar behaviour is mediated by a coordinated interaction between the passive, active, and neural subsystems.
During a normal, healthy gait cycle the foot transitions through four distinct functional phases:
0–8%
Initial Contact
Heel strike; subtalar joint in slight supination; lateral column contacts first to initiate shock attenuation.
8–30%
Loading Response
Controlled eversion unlocks the midfoot; the MLA descends ~4–6 mm; plantar fascia elongates; windlass disengaged.
30–50%
Midstance
Tibia advances over the planted foot; intrinsic muscles co-contract to resupinate the rearfoot and re-engage the windlass.
50–62%
Terminal Stance / Toe-Off
Hallux dorsiflexion tightens the plantar fascia via the windlass; the foot converts into a rigid propulsive lever.
The windlass mechanism is the hinge: hallux dorsiflexion winds the plantar fascia around the metatarsal heads, elevating the MLA, inverting the calcaneus, and stiffening the midfoot into a rigid lever for push-off. When intrinsic foot muscles are weak, this conversion fails.
07 — Pathomechanics
The Closed-Chain Kinetic Chain Collapse
Because the foot represents the sole point of contact with the ground during gait, any distal biomechanical deficit propagates up the closed kinetic chain, causing multi-segmental collapse from the calcaneus to the lumbar spine.
In individuals with functional pes planus the active subsystem lacks the tension needed to decelerate eversion and support the MLA during weight acceptance. The foot remains in a hyper-pronated, unlocked, soft state throughout the entire stance phase. The passive subsystem (ligaments, plantar fascia) must bear the entire structural load without muscular assistance — leading to chronic overstretching, microtearing, and complete failure of the windlass mechanism.
ReferenceSkeleton of the right foot, lateral aspect. Companion view to plate 290 — use to map how the talus, calcaneus and navicular displace in pes planus vs. the medial aspect shown above.
Gray's Anatomy (1918), plate 291 — public domain.
Foot & Ankle
Lever failure
NormalSupination at contact → controlled eversion → rapid resupination at terminal stance.
Pes PlanusHypermobile pronation; calcaneal eversion; persistent flatfoot throughout propulsion.
The Progressive Intrinsic Foot Muscle Training Protocol
To correct functional pes planus, rehabilitation must progress systematically from isolated, non-weight-bearing exercises to dynamic, multi-planar, functional loading. This allows the intrinsic foot musculature to develop base motor control and hypertrophy before being subjected to gravity and full bodyweight.
Stage 1
Absolute Zero — Seated Isolation & Sensory Integration
Weeks 1 – 4
Objective: establish neural pathway activation, isolate the intrinsic plantar muscles, and eliminate dominant compensatory movements from the extrinsic calf muscles (tibialis anterior, long toe flexors).
Seated Short Foot Exercise (Foot Doming)
Sit in a chair with hips, knees, and ankles bent to 90°; keep the bare foot flat on a high-friction surface. Shorten the foot in the anteroposterior plane by pulling the head of the 1st metatarsal toward the calcaneus, raising the MLA without curling or flexing the toes.
Video · 2:30Short Foot Exercise (Janda Protocol) — Dr. Donald Ozello, CCEDseminars. Watch the technique, the isometric hold, and the common toe-curling mistake to avoid.
Toe Dissociation Drills (Toe Yoga)
Independent control of the hallux vs. lesser toes. Lift the great toe while keeping digits 2–5 grounded, then reverse. The goal is cortical separation of flexor hallucis longus from flexor digitorum longus.
Video · 1:30Toe Separation Exercise — Yoga Tune Up. Demonstrates independent articulation of each toe and the spread-squeeze cycle.
Sensory & Mirror Therapy Integration
To accelerate motor learning and enhance the neural subsystem:
Mirror therapy — visual feedback of foot dome formation reinforces motor planning.
Textured surface training — proprioceptive enrichment via textured insoles or mats.
The patient must meet the following measurable benchmarks before progressing to weight-bearing work:
Hold time10-second isometric hold sustained without toe-claw compensation
Repetitions3 × 12 clean reps per foot
Toe dissociationHallux vs lesser-toe independent lift without FHL/FDL co-recruitment
Visual controlPatient can verbalise & visualise the dome in mirror feedback
Stage 2
Bilateral Closed-Chain Integration
Weeks 5 – 8
Objective: introduce weight-bearing forces so the arch learns to support the body under gravity while preserving active subsystem recruitment.
Standing Short Foot Exercise (Bilateral)
Stand upright, feet shoulder-width apart, weight evenly distributed. Execute the SFE simultaneously in both feet — lift the medial arches and draw the metatarsals toward the heels while maintaining neutral subtalar alignment.
Video · DemoShort Foot Exercise — The Proactive Athlete. Watch the standing bilateral dome formation with weight evenly distributed through the tripod.
Squat with Intrinsic Arch Preservation
Begin in a neutral posture with an active SFE dome in both feet. Perform a partial squat (progressing to 90° knee flexion) while maintaining arch height throughout the eccentric and concentric phases. Loss of the dome at depth signals the load ceiling.
Arch Raise Exercise (ARE) with Midfoot Resistance
A Thera-Band is anchored downward to the floor with a load of approximately 5 kgf, wrapped firmly over the midfoot (over the navicular tuberosity and cuboid). Perform a bilateral heel raise while actively contracting the intrinsic foot muscles to prevent the medial arch from collapsing under the downward tension.
Video · DemoArch Raises — chain-reaction demo. Shows how midfoot loading challenges the arch and the knee position that keeps the active subsystem recruited.
Stage 3
Unilateral Loading & Dynamic Balance
Weeks 9 – 12+
Objective: apply high postural demands; train the intrinsic foot muscles to dynamically stabilise the arch during single-leg tasks and integrate gains into real-world gait.
Single-Leg Stance SFE
Stand on one foot; establish an active short-foot dome; lift the opposite leg. Maintain MLA elevation and prevent the foot from rolling inward during natural postural sway.
Dynamic Reach (Star Excursion Balance Test)
Balancing on a single leg with an active short foot, reach the opposite leg as far as possible in three directions — anterior, posteromedial, posterolateral — lightly touching the floor with the toe before returning to start. The supporting foot must maintain its dome without collapse.
Video · DemoY-Balance Test — Physiotutors. Demonstrates the anterior, posteromedial, and posterolateral reach sequence and the stance-leg foot position required to keep the arch active.
Minimalist Shoe Walking (MSW) Transition
Minimalist shoes are characterised by a zero-drop heel-to-toe design, a wide toe box that allows the toes to splay, and a thin, flexible sole maximising sensory feedback. By removing artificial arch supports and thick cushioning, MSW increases the mechanical demands on the active plantar muscles, encouraging natural eversion-inversion cycles during daily walking.
Bone stress risk: MSW transition must be gradual to prevent bone stress injuries or tendon overload. Progress daily step volume in staged increments — abrupt jumps to full-day minimalist walking are a common cause of metatarsal and calcaneal stress reactions.
09 — Parameters
Stage Parameters at a Glance
A consolidated reference for clinical dosing across the three-stage protocol.
Phase
Posture
Exercises
Dosing
Biomechanical Target
Stage 1 Weeks 1 – 4
Non-weight-bearing / Seated
Seated SFE (Foot Doming); Toe Dissociation; Toes-Spread-Out; Isometric MTP Flexion
5 days/wk · 3 × 10–12 reps · 5–10 s hold · 2-min rest between sets. Mirror + textured surfaces.
Dynamic postural control during single-leg balance; real-world sensory integration; long-term intrinsic hypertrophy.
10 — References
Sources & Further Reading
Primary literature underpinning the clinical claims on this page.
[1]McKeon PO, Hertel J, Bramble D, Davis I. The foot core system: a new paradigm for understanding intrinsic foot muscle function. Br J Sports Med. 2015;49(5):290. bjsm.bmj.com
[3]Effects of Barefoot and Minimalist Footwear Strength-Oriented Training on Foot Structure and Function in Athletic Populations: A Systematic Review. PMC12609320
[4]Short foot exercises for flatfoot therapy: Status and prospects. PMC12775274
[5]Same article as [4] (PMC duplicate). PMC12775274
[6]Combined Use of Transcutaneous Electrical Nerve Stimulation and Short Foot Exercise Improves Navicular Height, Muscle Size, Function Mobility, and Risk of Falls in Healthy Older Adults. PMC9223504
[7]Effects of the Short Foot Exercise With Neuromuscular Electrical Stimulation on Navicular Height in Flexible Flatfoot in Thailand: A Randomized Controlled Trial. J Prev Med Public Health.jpmph.org
[8]Investigation of foot function, pain, flexibility and muscular performance levels according to the degree of pes planus in patients with plantar fasciitis. Turkish Journal of Sports Medicine. 2026;61(2). journalofsportsmedicine.org
[9]The extensibility of the plantar fascia influences the windlass mechanism during human running. Proc R Soc B. 2021;288(1943):20202095. royalsocietypublishing.org
[10]Effectiveness of Short Foot Exercise Combined With Proprioceptive Training Versus Short Foot Exercise Alone on Medial Longitudinal Arch Height and Balance in Individuals With Flexible Flat Foot. ResearchGate.researchgate.net
This page is for informational purposes only. For medical advice or diagnosis, consult a qualified professional.